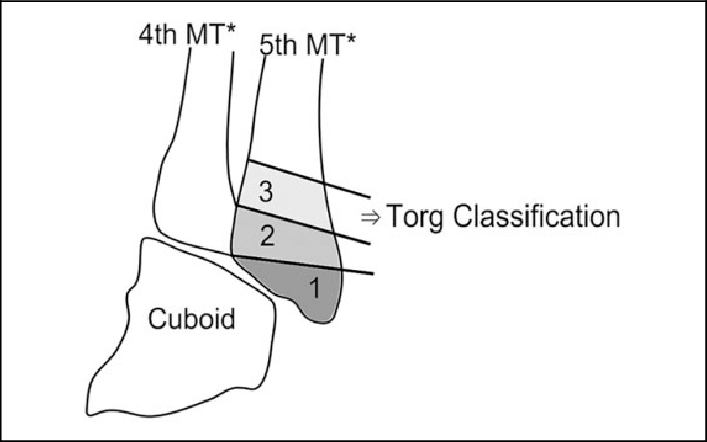
The Torg Classification, developed by Dr. J.W. Torg, is a classification system for fractures of the fifth metatarsal bone. This classification is primarily used to categorize fractures in athletes and guide treatment decisions based on the location and characteristics of the fracture.
The Torg Classification divides fifth metatarsal fractures into three zones:
Zone 1: Avulsion Fractures
- Involves an avulsion of the tuberosity of the fifth metatarsal due to pull of the peroneus brevis tendon.
- Often referred to as a “dancer’s fracture” or “pseudo-Jones fracture.”
- Typically has a good prognosis and usually heals well with conservative treatment.
Zone 2: Jones Fractures
- Occurs at the metaphyseal-diaphyseal junction of the fifth metatarsal, approximately 1.5 to 3 cm distal to the tuberosity.
- These fractures are more prone to delayed or non-union due to limited blood supply in this area.
- Often requires more aggressive treatment, including immobilization and sometimes surgical intervention.
Zone 3: Diaphyseal Fractures
- Involves fractures of the diaphysis (shaft) of the fifth metatarsal, occurring more distally than Zone 2.
- Generally has a better prognosis and often heals well with conservative treatment.