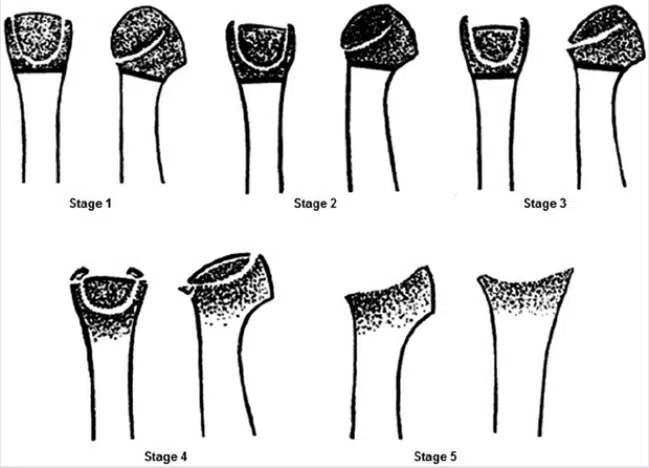
Smillie’s classification for Freiberg’s infarction involves five distinct stages:
Stage 1: Early Fissure and Sclerosis At the onset of Freiberg’s infarction, Stage 1 showcases a fissure in the epiphysis—this is the area of developing bone tissue—and an observable sclerosis between cancellous surfaces. Although symptoms may not be evident, this stage marks the beginning of the condition’s journey.
Stage 2: Absorption and Cartilage Sinking As the condition advances to Stage 2, there’s an absorption of cancellous tissue on the proximal side of the metatarsal head. This absorption prompts the sinking of the articular cartilage dorsally. At this point, patients may begin to experience limited motion and discomfort.
Stage 3: Further Absorption and Bony Projections Progressing to Stage 3, the absorption and sinking of the articular surface intensify. Bony projections emerge both medially and laterally, with the dorsal proximal metatarsal head developing exostosis—a bony outgrowth. This stage underscores the complexity of the condition.
Stage 4: Altered Anatomy and Fractures In Stage 4, the articular surface has sunken significantly, surpassing the point of easy restoration to normal anatomy. It’s important to note that fractures of the medial and lateral projections may occur, accentuating the severity of this stage.
Stage 5: Advanced Arthrosis The final frontier, Stage 5, witnesses the culmination of Freiberg’s infarction. Arthrosis takes center stage, leading to flattening and deformity of the metatarsal head. Interestingly, the plantar aspect retains the original cartilage contour, while the metatarsal shaft thickens and assumes a denser form.