The Hepple MRI Staging Classification is a significant framework used to categorize osteochondral lesions of the talus. These lesions involve damage to the cartilage and underlying bone of the ankle joint, often caused by trauma or repetitive stress. The Hepple classification assists in evaluating the severity of such lesions based on MRI findings, aiding in treatment planning and patient management.
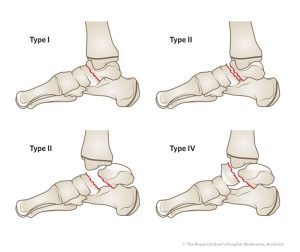
The Hepple MRI Staging Classification is divided into four distinct stages:
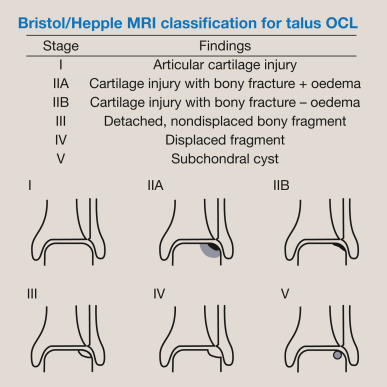
Stage I: This initial stage is characterized by a subchondral fracture, which appears as a signal change on MRI. The overlying cartilage may remain intact, and there might not be any noticeable separation between the cartilage and the bone. This stage indicates early damage, highlighting the importance of prompt diagnosis and intervention.
Stage II: In Stage II, there is evidence of cartilage separation from the underlying bone, often referred to as a “flap lesion.” This separation can be observed on MRI, and it indicates more significant damage to the osteochondral unit. Timely intervention at this stage can potentially prevent further deterioration.
Stage III: Continuing the progression, Stage III involves a partially detached cartilage fragment within the joint. This fragment is visible on MRI and is indicative of more advanced osteochondral damage. Treatment strategies at this stage may involve addressing the detached fragment to alleviate symptoms and prevent further complications.
Stage IV: The final stage of the Hepple classification represents complete detachment of the cartilage fragment within the joint. The detached fragment can be visualized on MRI and may even displace into the joint space. This stage underscores the urgency of appropriate management, which might include surgical options to restore joint function and prevent long-term consequences.