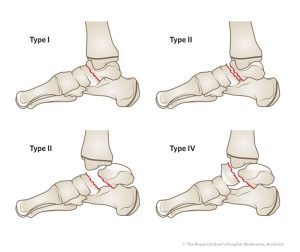
The Herscovici Classification for medial malleolar fractures takes expands from the classifications proposed by Müller et al and Pankovich and Shivaram, with a refined approach that groups fractures into four distinct patterns:
Type-A Fractures: At the simplest end of the spectrum, Type-A fractures involve avulsions of the malleolus tip. While these fractures may seem straightforward, their proper classification aids in tailoring appropriate treatment approaches.
Type-B Fractures: Type-B fractures occur between the tip of the malleolus and the level of the plafond. This pattern introduces a slightly more complex fracture location, necessitating careful consideration during diagnosis and treatment planning.
Type-C Fractures: The Type-C classification involves fractures occurring at the level of the plafond. This represents a pivotal point in the complexity of the fracture pattern and guides healthcare practitioners in devising effective management strategies.
Type-D Fractures: At the upper echelon of complexity, Type-D fractures extend vertically above the level of the plafond. These fractures demand meticulous attention due to their potential implications for treatment and healing.