Steve Edwards – Classic Article List (Updated August 2023)
Biomechanics
Hicks, J. H. (1954). The mechanics of the foot: II. The plantar aponeurosis and the arch. Journal of Anatomy, 88(Pt 1), 25.
Kirby, K. A. (2001). Subtalar joint axis location and rotational equilibrium theory of foot function. Journal of the American Podiatric Medical Association, 91(9), 465-487.
Thordarson, D. B., Schmotzer, H., Chon, J., & Peters, J. (1995). Dynamic support of the human longitudinal arch: A biomechanical evaluation. Clinical Orthopaedics and Related Research, 316, 165-172.
Equinus
Amis, J. (2014). The gastrocnemius: A new paradigm for the human foot and ankle. Foot and Ankle Clinics, 19(4), 637-647.
Amis, J. (2016). The split second effect: The mechanism of how equinus can damage the human foot and ankle. Frontiers in Surgery, 3, 38.
DiGiovanni, C. W., Kuo, R., Tejwani, N., et al. (2002). Isolated gastrocnemius tightness. Journal of Bone and Joint Surgery – American Volume, 84(6), 962-970.
Patel, A., & DiGiovanni, B. (2011). Association between plantar fasciitis and isolated contracture of the gastrocnemius. Foot and Ankle International, 32(1), 5-8.
First Ray
Johnson, C. H., & Christensen, J. C. (1999). Biomechanics of the first ray part I. The effects of peroneus longus function: A three-dimensional kinematic study on a cadaver model. Journal of Foot and Ankle Surgery, 38(5), 313-321.
Rush, S. M., Christensen, J. C., & Johnson, C. H. (2000). Biomechanics of the first ray. Part II: Metatarsus primus varus as a cause of hypermobility. A three-dimensional kinematic analysis in a cadaver model. Journal of Foot and Ankle Surgery, 39(2), 68-77.
Bierman, R. A., Christensen, J. C., & Johnson, C. H. (2001). Biomechanics of the first ray. Part III. Consequences of Lapidus arthrodesis on peroneus longus function: A three-dimensional kinematic analysis in a cadaver model. Journal of Foot and Ankle Surgery, 40(3), 125-131.
Roling, B. A., Christensen, J. C., & Johnson, C. H. (2002). Biomechanics of the first ray. Part IV: The effect of selected medial column arthrodeses. A three-dimensional kinematic analysis in a cadaver model. Journal of Foot and Ankle Surgery, 41(5), 278-285.
Johnson, C. H., & Christensen, J. C. (2005). Biomechanics of the first ray part V: The effect of equinus deformity: A 3-dimensional kinematic study on a cadaver model. Journal of Foot and Ankle Surgery, 44(2), 114-120.
Measurements
Lamm, B. M., Stasko, P. A., Gesheff, M. G., & Bhave, A. (2016). Normal foot and ankle radiographic angles, measurements, and reference points. Journal of Foot and Ankle Surgery, 55(5), 991-998.
Procedures
Lapidus, P. W. (1934). The operative correction of the metatarsus varus primus in hallux valgus. Surgery, Gynecology & Obstetrics, 58, 183-187.
Keller, W. L. (1904). The surgical treatment of bunions and hallux valgus. New York State Medical Journal, 80, 741-742.
Reverdin, J. (1881). Anatomic et operation de l’hallux valgus. International Medical Congress, 2, 408.
Laird, P., Silvers, S., & Somdahl, J. (1988). Two Reverdin-Laird osteotomy modifications for correction of hallux abducto valgus. Journal of the American Podiatric Medical Association, 78, 403.
Evans, D. (1975). Calcaneo-valgus. Journal of Bone and Joint Surgery, 57, 270-278.
Fractures
Lauge-Hansen, N. (1954). Fractures of the ankle. III. Genetic roentgenologic diagnosis of fractures of the ankle. American Journal of Roentgenology, Radium Therapy & Nuclear Medicine, 71(3), 456-471.
Lauge-Hansen, N. (1953). Fractures of the ankle. V. Pronation-dorsiflexion fracture. A.M.A. Archives of Surgery, 67(6), 813-820.
Lauge-Hansen, N. (1952). Fractures of the ankle. IV. Clinical use of genetic roentgen diagnosis and genetic reduction. A.M.A. Archives of Surgery, 64(4), 488-500.
Lauge-Hansen, N. (1950). Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations. Archives of Surgery, 60(5), 957-985.
Lauge-Hansen, N. (1949). Ligamentous ankle fractures; diagnosis and treatment. Acta Chirurgica Scandinavica, 97(6), 544-550.
Diabetes
Singh, N., Armstrong, D. G., & Lipsky, B. A. (2005). Preventing foot ulcers in patients with diabetes. JAMA, 293(2), 217-228.
Boulton, A. J. M., Vileikyte, L., Ragnarson-Tennvall, G., & Apelqvist, J. (2005). The global burden of diabetic foot disease. The Lancet, 366(9498), 1719-1724.
Lavery, L. A., Armstrong, D. G., & Harkless, L. B. (1996). Classification of diabetic foot wounds. Journal of Foot and Ankle Surgery, 35(6), 528-531.
Armstrong, D. G., Lavery, L. A., & Harkless, L. B. (1998). Validation of a diabetic wound classification system: The contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care, 21(5), 855-859.
Lipsky, B. A., Berendt, A. R., Deery, H. G., et al. (2004). Diagnosis and treatment of diabetic foot infections. Clinical Infectious Diseases, 39(7), 885-910.
Lipsky, B. A. (1997). Osteomyelitis of the foot in diabetic patients. Clinical Infectious Diseases, 25(6), 1318-1326.
Lew, D. P., & Waldvogel, F. A. (2004). Osteomyelitis. The Lancet, 364(9431), 369-379.
Frykberg, R. G., Zgonis, T., Armstrong, D. G., et al. (2006). Diabetic foot disorders: A clinical practice guideline (2006 revision). Journal of Foot and Ankle Surgery, 45(5), S1-S66.
Boulton, A. J. M., Armstrong, D. G., Albert, S. F., et al. (2008). Comprehensive foot examination and risk assessment. Diabetes Care, 31(8), 1679-1685.
Rogers, L. C., & Bevilacqua, N. J. (2010). Organized programs to prevent lower-extremity amputations. Journal of the American Podiatric Medical Association, 100(2), 101-104.
Cychosz, C. (2015). Preventive and therapeutic strategies for diabetic foot ulcers: A current concepts review. Foot & Ankle International, 36(8), 1071-1107.
Robbins, J. M., & Dillon, J. (2015). Evidence-based approach to advanced wound care products. Journal of the American Podiatric Medical Association, 105(5), 456-467.
Fedorko, L., Bowen, J. M., Jones, W., et al. (2016). Hyperbaric oxygen therapy does not reduce indications for amputation in patients with diabetes with nonhealing ulcers of the lower limb: A prospective, double-blind, randomized controlled clinical trial. Diabetes Care, 39(3), 392-399.
Sheehan, P., Jones, P., Caselli, A., et al. (2003). Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Diabetes Care, 26(6), 1879-1882.
Apelqvist, J., Bakker, K., Van Houtum, W. H., Nabuurs-Franssen, M. H., & Schaper, N. C. (1999). International consensus on the diabetic foot. Diabetes/Metabolism Research and Reviews, 15(Suppl 1), S6-S8.
Armstrong, D. G., Nguyen, H. C., Lavery, L. A., van Schie, C. H., Boulton, A. J., & Harkless, L. B. (2001). Off-loading the diabetic foot wound: A randomized clinical trial. Diabetes Care, 24(6), 1019-1022.
Attinger, C. E., Janis, J. E., Steinberg, J., Schwartz, J., Al-Attar, A., & Couch, K. (2006). Clinical approach to wounds: Debridement and wound bed preparation including the use of dressings and wound healing adjuvants. Plastic and Reconstructive Surgery, 117(7 Suppl), 72S-109S.
Jude, E. B., Oyibo, S. O., Chalmers, N., & Boulton, A. J. (2001). Peripheral arterial disease in diabetic and non-diabetic patients: A comparison of severity and outcome. Diabetes Care, 24(8), 1433-1437.
Kalani, M., Drismar, K., Fagrell, B., & Ostergren, J. (1999). Transcutaneous oxygen tension and toe blood pressure as predictors for outcome of diabetic foot ulcers. Diabetes Care, 22(1), 147-151.
Lavery, L. A., Armstrong, D. G., Peters, E. J. G., Lipsky, B. A., & Probe to Bone Consensus Group. (2007). Probe-to-bone test for diagnosing diabetic foot osteomyelitis: Reliable or relic? Diabetes Care, 30(2), 270-274.
Wagner, F. W. Jr. (1987). The diabetic foot. Orthopedics, 10(1), 163-172.
Wukich, D. K., Lowery, N. J., McMillen, R. L., & Frykberg, R. G. (2010). Postoperative infection rates in foot and ankle surgery: A comparison of patients with and without diabetes mellitus. The Journal of Bone and Joint Surgery. American volume, 92A(2), 287-295.
Tarsal Tunnel
Lam, S. J. (1967). Tarsal tunnel syndrome. The Journal of Bone and Joint Surgery. British volume, 49(1), 87-92. DOI: 0301-620X.49B1.87
Keck, C. (1962). The tarsal tunnel syndrome. The Journal of Bone and Joint Surgery. American volume, 44, 180-182.
Baxter, D. E., & Thigpen, C. M. (1984). Heel pain: Operative results. Foot & Ankle, 5(1), 16-25.
Baba, H., Wada, M., Annen, S., Azuchi, M., Imura, S., & Tomita, K. (1997). The tarsal tunnel syndrome: Evaluation of surgical results using multivariate analysis. International Orthopaedics, 21(2), 67-71.
Carrel, J. M., Davidson, D. M., & Goldstein, K. T. (1994). Observations on 200 surgical cases of tarsal tunnel syndrome. Clinics in Podiatric Medicine and Surgery, 11(4), 609-616.
Complex Regional Pain Syndrome (CRPS/RSD)
Anderson, D. J., & Fallat, L. M. (1999). Complex regional pain syndrome of the lower extremity: A retrospective study of 33 patients. The Journal of Foot and Ankle Surgery, 38(6), 381-387.
Shah, A., & Kirchner, J. S. (2011). Complex regional pain syndrome. Foot and Ankle Clinics, 16(2), 351-366.
Veldman, P. H., Reynen, H. M., Arntz, I. E., Goris, R. J., & Sigtermans, M. J. (1993). Signs and symptoms of reflex sympathetic dystrophy: A prospective study of 829 patients. The Lancet, 342(8878), 1012-1016.
Nerve Topics
Reilly, T. O., & Gerhardt, M. A. (2002). Anesthesia for foot and ankle surgery. Clinics in Podiatric Medicine and Surgery, 19(1).
Buxton, W. G., & Dominick, J. E. (2006). Electromyography and nerve conduction studies of the lower extremity: Uses and limitations. Clinics in Podiatric Medicine and Surgery, 23, 531-543.
Locke, R. K., & Locke, S. E. (1976). Nerve blocks of the foot. Annals of Emergency Medicine, 5(9), 698-702.
Kofoed, H. (1982). Peripheral nerve blocks at the knee and ankle in operations for common foot disorders. *Clinical Orthopaedics and Related Research, (168), 97-101.
Ankle Arthroscopy
Drez, D. J., Guhl, J. H., & Gollehon, D. L. (1981). Ankle arthroscopy: Technique and indications. Foot & Ankle, 2, 138-143.
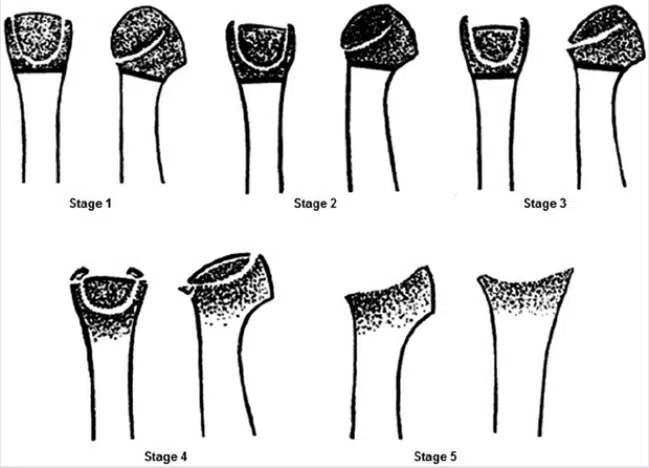
Bauer, M., Jonsson, K., & Linden, B. (1987). Osteochondritis dissecans of the ankle: A 20-year follow-up study. The Journal of Bone and Joint Surgery. British volume, 69(1), 93-96.
Branca, A., Di Palma, L., Bucca, C., et al. (1997). Arthroscopic treatment of anterior ankle impingement. Foot & Ankle International, 18(7), 418-423.
Glick, J. M., Morgan, C. D., Myerson, M. S., et al. (1996). Ankle arthrodesis using arthroscopic method: Long-term follow-up of 34 cases. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 12(4), 428-434.
Carlson, M. J., & Ferkel, R. D. (2013). Complications in ankle and foot arthroscopy. Sports Medicine and Arthroscopy Review, 21(2), 135-139.
Ferkel, R. D., & Scranton, P. E. Jr. (1993). Arthroscopy of the ankle and foot. The Journal of Bone and Joint Surgery. American volume, 75(8), 1233-1242.
Ferkel, R. D., & Fasulo, G. J. (1994). Arthroscopic treatment of ankle injuries. Orthopedic Clinics of North America, 25(1), 17-32.
Jaivin, J. S., & Ferkel, R. D. (1994). Arthroscopy of the foot and ankle. Clinics in Sports Medicine, 13(4), 761-783.
Stetson, W. B., & Ferkel, R. D. (1996). Ankle arthroscopy: I. Technique and complications. Journal of the American Academy of Orthopaedic Surgeons, 4(1), 17-23.
Stetson, W. B., & Ferkel, R. D. (1996). Ankle arthroscopy: II. Indications and results. Journal of the American Academy of Orthopaedic Surgeons, 4(1), 24-34.
Williams, M. M., & Ferkel, R. D. (1998). Subtalar arthroscopy: Indications, technique, and results. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 14(4), 373-381.
Ferkel, R. D., & Hewitt, M. (2005). Long-term results of arthroscopic ankle arthrodesis. Foot & Ankle International, 26(4), 275-280.
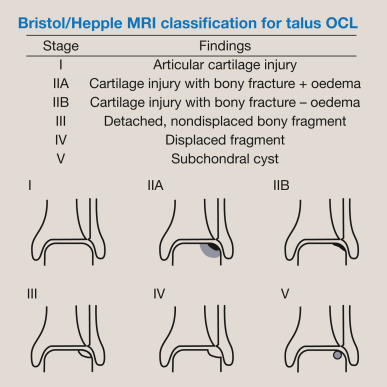
Ferkel, R. D., Zanotti, R. M., Komenda, G. A., Sgaglione, N. A., Cheng, M. S., Applegate, G. R., & Dopirak, R. M. (2008). Arthroscopic treatment of chronic osteochondral lesions of the talus: Long-term results. The American Journal of Sports Medicine, 36(9), 1750-1762.
Hindfoot and Ankle Arthritis
Ahmad, J., & Pedowitz, D. (2012). Management of the Rigid Arthritic Flatfoot in Adults: Triple Arthrodesis. Foot & Ankle Clinics, 17(2), 337-349.
Aronow, M. S., & Hakim-Zargar, M. (2007). Management of Hindfoot Disease in Rheumatoid Arthritis. Foot & Ankle Clinics, 12(3), 455-474.
Astion, D. J., Deland, J. T., Otis, J. C., & Kenneally, S. (1997). Motion of the Hindfoot after Simulated Arthrodesis. The Journal of Bone and Joint Surgery. American volume, 79(2), 241-246.
Bibbo, C., Anderson, R. B., & Davis, W. H. (2001). Complications of Midfoot and Hindfoot Arthrodesis. Clinical Orthopaedics and Related Research, (391), 45-59.
Buck, P., Morrey, B. F., & Chao, E. Y. (1987). The Optimum Position of Arthrodesis of the Ankle: A Gait Study of the Knee and Ankle. The Journal of Bone and Joint Surgery. American volume, 69, 1052-1062.
Chen, C. H., Huang, P. J., Chen, T. B., et al. (2001). Isolated Talonavicular Arthrodesis for Talonavicular Arthritis. Foot & Ankle International, 22, 633-636.
Chuinard, E., & Peterson, R. (1983). Distraction-Compression Bone-Graft Arthrodesis of the Ankle. The Journal of Bone and Joint Surgery. American volume, 45, 481-490.
Coester, L. M., Saltzman, C. L., Leupold, J., & Pontarelli, W. (1989). Long-term Results Following Ankle Arthrodesis for Post-traumatic Arthritis. The Journal of Bone and Joint Surgery. American volume, 83(2), 219-228.
Cooper, P. S. (2001). Complications of Ankle and Tibiotalocalcaneal Arthrodesis. Clinical Orthopaedics and Related Research, (391), 33-44.
Dalziel, R., Thornhill, T. S., & Thomas, W. H. (1982). Isolated Talonavicular Fusion for Hindfoot Arthritis. Orthopedic Trans., 6, 341.
Dennis, M. D., & Tullos, H. S. (1980). Blair Tibiotalar Arthrodesis for Injuries to the Talus. The Journal of Bone and Joint Surgery. American volume, 62, 103-117.
Donatto, K. C. (1998). Arthritis and Arthrodesis of the Hindfoot. Clinical Orthopaedics and Related Research, (349), 81-92.
Fallace, J. J., Leopold, S. S., & Brage, M. E. (2000). Extended Hindfoot Fusions and Pantalar Fusions. History, Biomechanics and Clinical Results. Foot & Ankle Clinics, 5(4), 777-798.
Greisberg, J., & Sangeorzan, B. (2007). Hindfoot Arthrodesis. The Journal of the American Academy of Orthopaedic Surgeons, 15, 65-71.
Glissan, D. J. (1949). The Indications for Inducing Fusion at the Ankle Joint by Operation with Description of Two Successful Techniques. Aust NZ J Surg., 19, 64-71.
Horwitz, T. (1942). The Use of the Transfibular Approach in the Arthrodesis of the Ankle. The American Journal of Surgery, 60, 550-552.
Joseph, T. N., & Myerson, M. S. (2005). Correction of Multiplanar Hindfoot Deformity with Osteotomy, Arthrodesis, and Internal Fixation. Instr Course Lect., 54, 269-276.
Khoury, N. J., elKhoury, G. Y., Saltzman, C. L., & Brandser, E. A. (2003). Intraarticular Foot and Ankle Injections to Identify Source of Pain before Arthrodesis. AJR. American Journal of Roentgenology, 167(3), 669-673.
Lorthioir, J. (1911). Huit ras d’arthrodese du pied avec extirpation temporaire de l’astragala. Ann Soc Belge Chir., 11, 184-187.
Lundeen, R. O. (1994). Arthroscopic Fusion of the Ankle and Subtalar Joint. Clinical Podiatric Medicine and Surgery, 11(3), 395-406.
Mandracchia, V. J., Mandi, D. M., Nickles, W. A., et al. (2004). Pantalar Arthrodesis. Clinical Podiatric Medicine and Surgery, 21, 461-470.
Moss, M., Radack, J., & Rockett, M. S. (2004). Subtalar Arthrodesis. Clinical Podiatric Medicine and Surgery, 21(2), 179-201.
Muir, D. C., Amendola, A., & Saltzman, C. L. (2002). Long-term Outcome of Ankle Arthrodesis. Foot & Ankle Clinics of North America, 7(4), 703-708.
Myerson, M. S., & Quill, G. (1991). Ankle Arthrodesis: A Comparison of an Arthroscopic and an Open Method of Treatment. Clinical Orthopaedics and Related Research, 268, 84-95.
Nickisch, F., Avilucea, F. R., Beals, T., & Saltzman, C. (2011). Open Posterior Approach for Tibiotalar Arthrodesis. Foot & Ankle Clinics, 16(1), 103-114.
Nuesch, C., Barg, A., Pagenstert, G. I., & Valderrabano, V. (2013). Biomechanics of Asymmetric Ankle Osteoarthritis and Its Joint-Preserving Surgery. Foot & Ankle Clinics, 18(3), 427-436.
Rammelt, S., & Zwipp, H. (2013). Corrective Arthrodesis and Osteotomies for Post-Traumatic Hindfoot Malalignment: Indications, Techniques, Results. International Orthopaedics, 37(9), 1707-1717.
Ryerson, E. W. (1923). Arthrodesing Operations on the Foot. The Journal of Bone and Joint Surgery. American volume, 5, 453-471.
Saltzman, C. L., Salamon, M. L., Blanchard, G. M., et al. (2005). Epidemiology of Ankle Arthritis: Report of a Consecutive Series of 639 Patients from a Tertiary Orthopaedic Center. Iowa Orthopedic Journal, 25, 444-446.
Snedeker, J. G., Wirth, S. H., & Espinosa, N. (2012). Biomechanics of the Normal and Arthritic Ankle Joint. Foot & Ankle Clinics, 17(4), 517-528.
Thomas, R. H., & Daniels, T. R. (2003). Current Concepts Review: Ankle Arthritis. The Journal of Bone and Joint Surgery. American volume, 85, 923-936.
Wapner, K. L. (1998). Triple Arthrodesis in Adults. Journal of the American Academy of Orthopaedic Surgeons, 6(3), 188-196.
Wilson, P. D. (1927). Treatment of the Fractures of OS Calcis by Arthrodesing of the Subtalar Joint: A Report on 26 Cases. Journal of the American Medical Association, 89, 1676-1683.
Non-Unions Delayed Unions
Bolhofner, B. R., Finnergan, M., & Landy, D. W. (2010). Chapter 14: Nonunions and Malunions. In A. H. Schmidt & D. C. Teague (Eds.), Orthopaedic Knowledge Update: Trauma 4 AAOS.
Chiodo, C. P., Cicchinelli, L., Kadakia, A. R., Schuberth, J., & Weil Jr., L. (2010). Malunion and Nonunion in Foot and Ankle Surgery. Foot & Ankle Specialist, 3(4), 194-200.
Hak, D. J., Fitzpatrick, D., Bishop, J. A., Marsh, J. L., Tilp, S., Schnettler, R., Simpson, H., & Alt, V. (2014). Delayed Union and Nonunions: Epidemiology, Clinical Issues, and Financial Aspects. Injury, 45(Suppl 2), S3-S7.
Mandracchia, V. J., Nickles, W. A., Mandi, D. M., Jaeger, A. J., & Sanders, S. M. (2004). Treatment of Nonunited Hindfoot Fusions. Podiatric Medical and Surgical Journal, 21(3), 417-439.
Marsh, D. (1998). Concepts of Fracture Union, Delayed Union, and Nonunion. Clinical Orthopaedics and Related Research, 355(Suppl), S22-S30.
Martone, J., Poel, L. V., & Levy, N. (2012). Complications of Arthrodesis and Nonunion. Clinical Podiatry and Medical Surgery, 29(1), 11-18.
Molloy, A. P., Roche, A., & Narayan, B. (2009). Treatment of Nonunion and Malunion of Trauma of the Foot and Ankle Using External Fixation. Foot and Ankle Clinics, 14(3), 563-587.
Schoelles, K., Snyder, D., Kaczmarek, J., Kuserk, E., Erinoff, E., Turkelson, C., & Coates, V. (2005). The Role of Bone Growth Stimulating Devices and Orthobiologics in Healing Nonunion Fractures. AHRQ Technology Assessments / Agency for Healthcare Research and Quality.
Shibuya, N., Humphers, J. M., Fluhman, B. L., & Jupiter, D. C. (2013). Factors Associated with Nonunion, Delayed Union, and Malunion in Foot and Ankle Surgery in Diabetic Patients. The Journal of Foot & Ankle Surgery, 52(2), 207-211.
Thevendran, G., Younger, A., & Pinney, S. (2012). Current Concepts Review: Risk Factors for Nonunions in Foot and Ankle Arthrodeses. Foot & Ankle International, 33(11), 1031-1040.
Surgical Site Infections
Akinyoola, A. L., Adegbehingbe, O. O., & Odunsi, A. (2011). Timing of Antibiotic Prophylaxis in Tourniquet Surgery. Journal of Foot and Ankle Surgery, 50(4), 374-376.
Bibbo, C., Patel, D. V., Gehrmann, R. M., & Lin, S. S. (2005). Chlorhexidine Provides Superior Skin Decontamination in Foot and Ankle Surgery: A Prospective Randomized Study. Clinical Orthopaedics and Related Research, 438, 204-208.
Deacon, J. S., Wertheimer, S. J., & Washington, J. A. (1996). Antibiotic Prophylaxis and Tourniquet Application in Podiatric Surgery. Journal of Foot and Ankle Surgery, 35(4), 344-349.
Kubota, A., Nakamura, T., Miyazaki, Y., Sekiguchi, M., & Suguro, T. (2012). Perioperative Complications in Elective Surgery in Patients with Rheumatoid Arthritis Treated with Biologics. Modern Rheumatology, 22(6), 844-848.
Mote, G. A., & Malay, D. S. (2010). Efficacy of Power-Pulsed Lavage in Lower Extremity Wound Infections: A Prospective Observational Study. Journal of Foot and Ankle Surgery, 49(2), 135-142.
Rabih, O. D., & Darouiche, R. O. et al. (2010). Chlorhexidine–Alcohol versus Povidone–Iodine for Surgical-Site Antisepsis. New England Journal of Medicine, 362(1), 18-26.
Zgonis, T., Jolly, G. P., & Garbalosa, J. C. (2004). The Efficacy of Prophylactic Intravenous Antibiotics in Elective Foot and Ankle Surgery. Journal of Foot and Ankle Surgery, 43(2), 97-103.
Paediatric Flatfoot
Blitz, N. M., Stabile, R. J., Giorgini, R. J., & DiDomenico, L. A. (2010). Flexible Pediatric and Adolescent Pes Planovalgus: Conservative and Surgical Treatment Options. Clinics in Podiatric Medicine and Surgery, 27(1), 59-111.
Cappello, T., & Song, K. M. (1998). Determining Treatment of Flatfeet in Children. Current Opinion in Pediatrics, 10, 77-81.
Dare, D. M., & Dodwell, E. R. (2014). Pediatric Flatfoot: Cause, Epidemiology, Assessment and Treatment. Current Opinion in Pediatrics, 26(1), 93-100.
Evans, D., & Cardiff, W. (1975). Calcaneo-Valgus Deformity. Journal of Bone and Joint Surgery (British Volume), 57(3), 270-278.
Giannini, S., Ceccarelli, F., Benedetti, M. G., et al. (2001). Surgical Treatment of Flexible Flatfoot in Children: A Four Year Follow Up Study. Journal of Bone and Joint Surgery (American Volume), 83(Suppl 2, Pt 2), 73-79.
Grice, D. S. (1952). An Extra-Articular Arthrodesis of the Subastragalar Joint for Correction of Paralytic Flat Feet in Children. Journal of Bone and Joint Surgery (American Volume), 34, 972-940.
Harris, E. J., Vanore, J. V., Thomas, J. L., Kravitz, S. R., Mendelson, S. A., Mendicino, R. W., Silvani, S. H., & Couture Gassen, S. (2004). Diagnosis and Treatment of Pediatric Flatfoot (Clinical Practice Guideline). Journal of Foot and Ankle Surgery, 43(6), 341-370.
Herndon, C. H., & Heyman, C. H. (1963). Problems in the Recognition and Treatment of Congenital Convex Pes Valgus. Journal of Bone and Joint Surgery (American Volume), 45, 413-429.
Labovitz, J. M. (2006). The Algorithmic Approach to Pediatric Flexible Pes Planovalgus. Clinics in Podiatric Medicine and Surgery, 23(1), 57-76.
Mahan, K. T., & McGlamry, E. D. (1987). Evans Calcaneal Osteotomy for Flexible Pes Valgus Deformity. A Preliminary Study. Clinics in Podiatric Medicine and Surgery, 4, 137–151.
Mosca, V. S. (1995). Flexible Flatfoot and Skewfoot. An Instructional Course Lecture. Journal of Bone and Joint Surgery (American Volume), 77, 1937-1945.
Patterson, W. R., Fritz, D. A., & Smith, W. S. (1968). The Pathologic Anatomy of Congenital Convex Pes Valgus. Journal of Bone and Joint Surgery (American Volume), 50, 458.
Pavone, V., et al. (2013). Calcaneo-Stop Procedure in the Treatment of Juvenile Symptomatic Flatfoot. Journal of Foot and Ankle Surgery, 52, 444–447.
Rodriguez, N., & Volpe, R. G. (2010). Clinical Diagnosis and Assessment of the Pediatric Pes Planovalgus Deformity. Clinics in Podiatric Medicine and Surgery, 27(1), 43-58.
Roye, D. P., & Raimondo, R. A. (2000). Surgical Treatment of the Child’s and Adolescent’s Flexible Flatfoot. Clinics in Podiatric Medicine and Surgery, 17(3), 515-530.
Scranton, P. E. (1987). Treatment of Symptomatic Talocalcaneal Coalition. Journal of Bone and Joint Surgery (American Volume), 69, 533–539.
Silvani, S. H. (1987). Congenital Convex Pes Valgus. Clinics in Podiatric Medicine and Surgery, 4, 163-173.
Sullivan, J. A. (1999). Pediatric Flatfoot: Evaluation and Management. Journal of the American Academy of Orthopaedic Surgeons, 7, 445-453.
Tachdjian, M. O. (1972). Congenital Convex Pes Valgus. Orthopedic Clinics of North America, 3, 131–148.
Total Ankle Arthroplasty
Bibbo, C. (2012). Controversies in Total Ankle Replacement. Clinics in Podiatric Medicine and Surgery, 30, 21-34.
Conti, S. F., & Wong, Y. S. (2002). Complications of Total Ankle Replacement. Foot and Ankle Clinics of North America, 7, 791-807.
DiDomenico, L., & Anania, M. (2011). Total Ankle Replacements: An Overview. Clinics in Podiatric Medicine and Surgery, 28(4), 727-744.
Esparragoza, L., Vidal, C., & Vaquero, J. (2011). Comparative Study of the Quality of Life Between Arthrodesis and Total Arthroplasty Substitution of the Ankle. Journal of Foot & Ankle Surgery, 50, 383-387.
Gougoulias, N., Khanna, A., & Maffulli, N. (2009). History and Evolution in Total Ankle Arthroplasty. British Medical Bulletin, 89(1), 111-151.
Gougoulias, N., & Maffulli, N. (2012). History of Total Ankle Replacement. Clinics in Podiatric Medicine and Surgery, 30, 1-20.
Guyer, A., & Richardson, E. (2008). Current Concepts Review: Total Ankle Arthroplasty. Foot & Ankle International, 29, 256.
Henne, T., & Anderson, J. (2002). Total Ankle Arthroplasty: A Historical Perspective. Foot and Ankle Clinics of North America, 7, 695-702.
Lagaay, P., & Schuberth, J. (2010). Analysis of Ankle Range of Motion and Functional Outcome Following Total Ankle Arthroplasty. Journal of Foot & Ankle Surgery, 49, 147-151.
Overly, B. (2012). Total Ankle Replacement: A Historical Perspective. Clinics in Podiatric Medicine and Surgery, 29(4), 547-570.
Roukis, T., & Prissel, M. (2013). Registry Data Trends of Total Ankle Replacement Use. Journal of Foot & Ankle Surgery, 52, 728-735.
Valderrabano, V., Nigg, B., von Tscharner, V., Frank, C., & Hintermann, B. (2007). Total Ankle Replacement in Ankle Osteoarthritis: An Analysis of Muscle Rehabilitation. Foot & Ankle International, 28(2), 282-291.
Valderrabano, V., Pagenstert, G., Muller, A., Paul, J., Henninger, H., & Barg, A. (2012). Mobile- and Fixed-Bearing Total Ankle Prostheses. Is There Really a Difference? Foot & Ankle Clinics, 17(4), 565-585.
Zaidi, R., Cro, S., Gurusamy, K., Siva, N., Macgregor, A., Henricson, A., & Goldberg, A. (2013). The Outcome of Total Ankle Replacement: A Systematic Review and Meta-analysis. The Bone & Joint Journal, 95-B(11), 1500-1507.