Weber fractures are a classification system for fractures of the ankle, specifically the fibula bone. The Weber classification system is based on the location of the fracture relative to the ankle joint and the degree of displacement of the fracture.
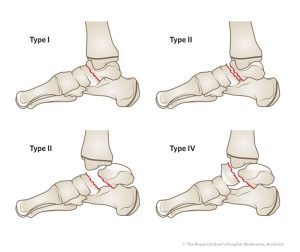
There are three types of Weber fractures:
- Weber A: This is a fracture of the fibula that occurs below the level of the ankle joint. The ankle joint itself is not affected. The fracture may be non-displaced (the bone is still aligned properly) or displaced (the bone is out of alignment). This type of fracture is usually treated with immobilization and rest.
- Weber B: This is a fracture of the fibula that occurs at the level of the ankle joint. The ankle joint is also affected, as the fracture extends into the ligaments that connect the fibula to the tibia bone. This type of fracture is typically treated with immobilization, rest, and sometimes surgery to realign the bones and stabilize the joint.
- Weber C: This is a fracture of the fibula that occurs above the level of the ankle joint, often at the level of the syndesmosis (the joint between the tibia and fibula bones). The ankle joint is not usually affected, but there may be significant ligament damage. This type of fracture is often treated with surgery to realign the bones and stabilize the joint.
Overall, the Weber classification system is a useful tool for healthcare professionals in assessing and managing ankle fractures. Treatment options for Weber fractures may include immobilization with a cast or brace, surgery to realign the bones and stabilize the joint, and physical therapy to restore range of motion and strength to the ankle.